


How OCT-guided diagnosis is reshaping the BCC pathway

Fewer biopsies.
Faster decisions.
The same clinical outcomes.
A randomised controlled trial published in The Lancet Oncology found that OCT-BCC diagnosis avoided a diagnostic biopsy in 66% of Basal Cell Carcinoma patients — with non-inferior clinical outcomes at 12 months, and a lower cost per lesion.
THE DIAGNOSTIC PATHWAY
A structural challenge for every busy clinic
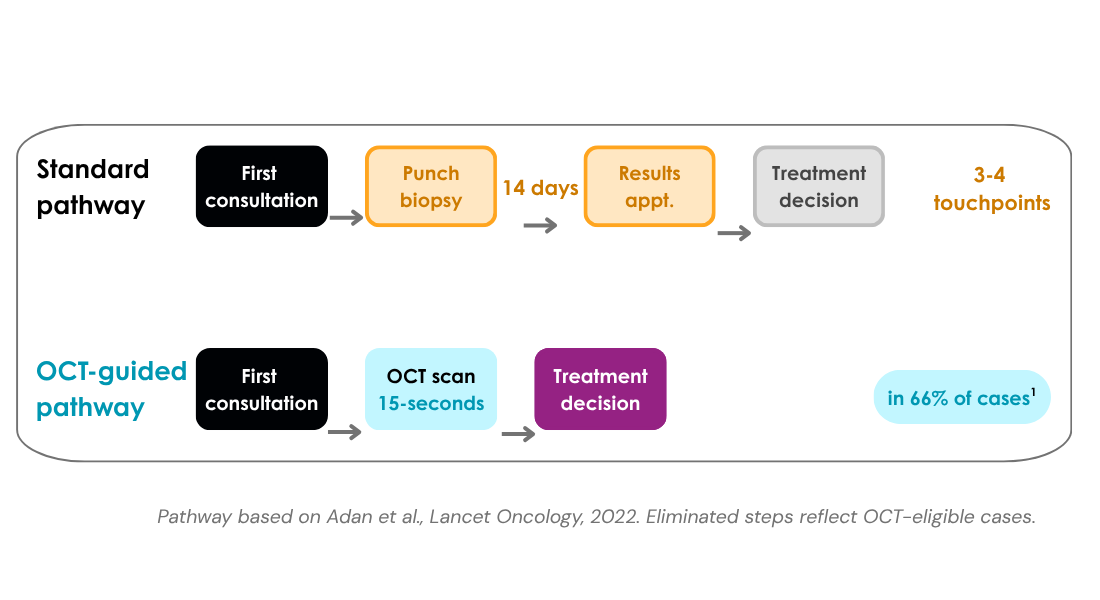
The established route to a BCC diagnosis follows a predictable sequence: initial consultation, punch biopsy, histopathology processing, results appointment, and — finally — treatment planning. Each step is clinically appropriate. Collectively, they consume appointment capacity that cannot be directed toward new patients, lengthen time to treatment, and require the patient to undergo an invasive procedure before a treatment decision can be made.
OCT BCC diagnosis changes this sequence. In 66% of cases, a 15-second non-invasive scan at first consultation is sufficient to confirm or exclude BCC — removing the biopsy, the waiting period, and the results appointment from the pathway entirely.
The data is now clear
Level 1 Clinical Evidence
A multicentre randomised controlled trial — the highest level of clinical evidence — assessed OCT-guided diagnosis against the established biopsy pathway in 598 patients across three specialist centres. The results were published in The Lancet Oncology in 2022.
-

66% of diagnostic biopsies avoided with OCT-guided diagnosis
Adan et al., Lancet Oncology, 2022¹
-

€69 lower cost per lesion in the OCT-guided pathway vs. biopsy
598 patients, 3 centres, RCT¹
-

12 months – equivalent clinical outcomes at follow-up — non-inferiority demonstrated
Adan et al., Lancet Oncology, 2022¹
“In 66% of patients, a biopsy could be avoided, thus minimising treatment delay and avoiding an invasive procedure.”
Adan et al. Lancet Oncology, 2022; 23(8):1087–1096
Guideline-endorsed clinical practice — OCT is now included in the European Consensus BCC Guidelines (2023) and in national dermatology guidelines across Europe, including Germany, the UK, Denmark, and The Netherlands.
Designed for speed, confidence and efficiency
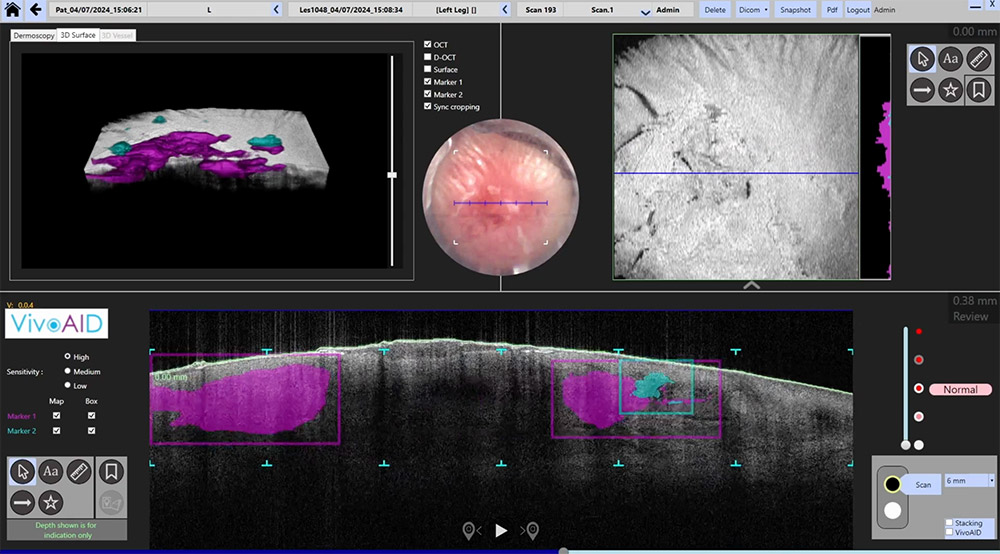
VivoSight Dx Pro with VivoAID
VivoSight Dx Pro delivers a full 3D OCT scan in 15 seconds, non-invasively, at the point of care. The 6mm × 6mm field of view and depth penetration of greater than 1mm provide the sub-surface structural information required to characterise BCC and determine subtype — in the same consultation in which the lesion is first examined.
VivoAID, the integrated AI assistant*, analyses each scan and directs clinical attention to areas of interest before review. This directly reduces image interpretation time and lowers the learning curve for clinicians new to OCT imaging.
- 15-second full 3D scan — No skin preparation required. Acquired at the point of care.
- 6 × 6mm field of view — Entire lesion visualised in a single scan. Greater than 1mm depth penetration.
- AI-assisted image analysis — VivoAID markers placed before clinical review, directing attention to areas of diagnostic interest.
- CE-marked Class IIa medical device — Cited in over 800 peer-reviewed publications worldwide.
“The number of biopsies needed are reduced dramatically. The AI helps me even as a very experienced doctor to find areas where I need to take a closer look.
Dr. Uwe Paasch, Professor of Dermatology, University of Leipzig, Germany.
See VivoSight Dx Pro in your clinical context
Request an online demonstration with a VivoSight clinical specialist. No obligation.
¹ Adan F. et al. ‘Optical coherence tomography versus punch biopsy for diagnosis of basal cell carcinoma: a multicentre, randomised, non-inferiority trial.’ Lancet Oncology. 2022;23(8):1087–1096. doi: 10.1016/S1470-2045(22)00347-3. RCT, 598 patients, 3 centres.
² European Consensus BCC Guidelines (2023). National guideline applicability varies by market — contact your regional VivoSight representative for local guidance.
VivoSight Dx Pro is a CE-marked Class IIa medical device under MDR (EU 2017/745).
* VivoAID is provided solely as an educational aid and has not been approved for use in the clinical pathway. OCT image analysis and interpretation remain the clinical responsibility of the physician.